|
||||||||||||||
 |
||||||||||||||
Sialendoscopy
Standard diagnostic approaches The classical investigation methods of salivary glands are radiography, including X-rays, ultrasound, CT scan and sialography, which up to now is considered as the gold standard for evaluation of the ductal system.(3) Ultrasound remains an excellent primary diagnostic method for the detection of salivary stones, however calculi with a size less than 3 mm can hardly be visualized.(4) Another new non invasive diagnostic option is nuclear magnetic resonance tomography, which provides scans of the salivary ducts by opacification of the natural salivary pathway without the need for administration of contrast medium and without exerting the patient to ionising irradiation.(5) These procedures aim to visualize the ductal system for the diagnosis of obstructive pathologies, typically stones or other rarer diseases.
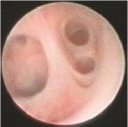
Diagnostic Sialendoscopy Introduction The new endoscopic techniques described(6,7) and the specific instrument set we designed and developed in collaboration with Karl Storz, allows almost complete exploration of the ductal system (main duct, secondary and tertiary branches), (Figure 1) mainly because of the small diameter of the scopes (0.9 and 1.3 mm). Over the last 450 endoscopies performed, diagnostic sialendoscopy could be achieved in 98% of cases. Rare limitations include convoluted sections that are impassable with a rigid endoscope.(8,9)Mobility of the endoscope is also limited at the distal end of the gland. Sialendoscopy provides direct, reliable information about most pathologies and reduces the need for radiological investigations.
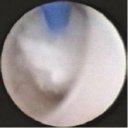
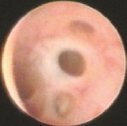
Pathological findings
Clinical Consequences of Sialolithiasis Sialolithiasis results in a mechanical obstruction of the salivary duct, causing recurrent glandular swellings during meals, transitory or complicated by bacterial infections accompanied by fever, purulent discharge at the papilla and painful glandular swelling. In the classical attitude, proximal stones close to the papilla are simply extracted,(14) whereas glandular resection is indicated for deeply located stones. In submandibular glands, sialolithiasis surgery still represents 70% to 90% of all actual indications(15) for surgery, although several reports demonstrate a relatively high rate of complications including neurologic damages. Parotidectomy is rarely performed for inflammatory conditions in parotid glands, because it remains a tedious procedure and carries involves a higher incidence of post-operative paresis.(16) A possible reason for this high rate of submandibular resections might be the common belief that a gland suffering from long standing sialolithiasis is no longer functional. In a clinical- histopathological study(17) on 48 patients afflicted with sialolithiasis treated with glandular resection, one half of the patients had subnormal histology patterns, and there was no correlation between the number of infectious episodes and the alteration of the gland. Therefore, numerous infectious episodes or a long duration of symptoms cannot be used to predict the degree of glandular alteration, and thus a conservative attitude towards sialolithiasis appears justified. In search of conservative approaches towards sialolithiasis, a new technique was developed in the 1990s, namely extracorporeal lithotripsy.(18) Success rates vary from 40% to 75% for the submandibular and parotid glands, respectively. Performed on an outpatient basis, this technique is now widely practiced but often requires multiple sessions. The main problem remainsthe clearance of fragments, which is incomplete and could become the cause of recurrent sialolithiasis. Interventional sialendoscopy, as described hereafter, allows avoidance of these problems.
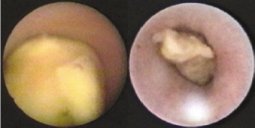
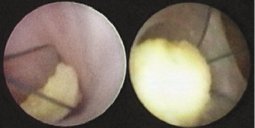
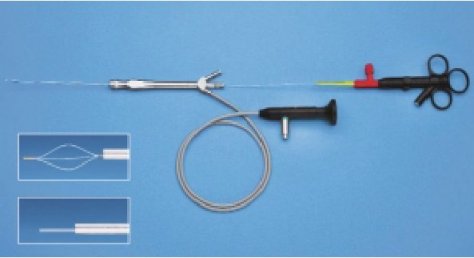
Interventional Sialendoscopy The attitude is the same for the submandibular8 and parotid glands,(9) although the diameter of the ductal system is smaller in the parotid duct. For small stones less than 4mm in diameter in submandibular cases (figure 6) and less than 3mm for parotid cases (figure 7), extraction is performed with custom designed wire baskets of various sizes (figure 8).
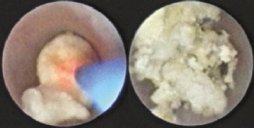
In cases of bigger stones, a prior fragmentation is necessary, using a laser system (figures 9 and 10), or an eventual extracorporal lithotriptor. Stenoses are treated with metallic dilators or with balloon catheters. It is important to emphasize that these techniques of fragmentation and stone retrieval are performed under endoscopic control, as described by others.(19)We do not recommend the semi blind technique, consisting of introducing the basket after the removal of the optic fiber because of its lack of precision and potential danger of perforation. In recent published studies, we detailled our results with an overall success rate of 83%.(8,9)
Technique Indications and Contraindications The indications for sialendoscopy are all salivary gland swellings of unclear origin.(20) There are no specific contraindications, mostly because sialendoscopy is a minimally invasive outpatient procedure performed under local anesthesia. Even children,(21) or elderly patients can benefit from this technique. Despite its apparent simplicity, interventional sialendoscopy is a technically challenging procedure. Operating the rigid sialendoscope is delicate, requires experience and might be hazardous due to theoretical risks of perforation and vascular or neural damage. Progression in the canal should be performed only under adequate vision. Perforations of iatrogenic origin can lead to diffuse swellings of the floor of mouth, with potential risks of life-threatening swellings. Operative technique Sialendoscopy can be done as an outpatient procedure with the patient sitting in a chair or partially recumbent. Anesthesia is purely local. Progressive dilatation of the papilla is performed with salivary sounds of progressively larger diameters. Endoscopy is performed with progressive endoluminal irrigation using a local anesthetic solution. The diagnostic and interventional sialendoscope (1.33mm2 surface, 1.3mm diameter) (figure 11) provides excellent vision and is recommended both for diagnostic and interventional procedures as it has a rinsing channel as well as a working channel.
Limitations The writhing course of the canal puts certain limitations on semi-rigid endoscopy, especially in cases of sharply bent curvatures. Also, maneuvering within the small salivary ducts has to be absolutely atraumatic because of possible ductal perforation of yet uncertain consequences. Significant trauma to the ductal wall could result in latter stenosis. Marsupialization of the ductal papillae should either be completely avoided, or kept as small as possible to prevent retrograde passage of air and aliments. Conclusion Diagnostic sialendoscopy is a low morbidity minimally invasive technique, which may become the investigational procedure of choice for salivary duct pathologies. Interventional sialendoscopy allows the treatment of sialolithasis and stenosis, and help therefore to prevent salivary gland excisions.
References
|
||||||||||||||||||||||
© Sialendoscopy.net |
||||||||||||||||||||||